.
.
Summary: The ventilatory effect of High Velocity Nasal Insufflation versus Non-invasive Positive Pressure Ventilation in the treatment of acute hypercapnic respiratory failure in patients with AECOPD.
Topic: Egyptian Studies
Ibrahim BM, Abdelfatah MT, Al-Sherif M et al. The ventilatory effect of High Velocity Nasal Insufflation versus Non-invasive Positive Pressure Ventilation in the treatment of acute hypercapnic respiratory failure in patients with AECOPD. MJMR, Vol. 35, No. 2, 2024, pages (21-31) DOI: 10.21608/MJMR.2024.291881.1713
Ibrahim and colleagues conducted a single center, randomized study of acute hypercapnic respiratory failure patients presenting to Cardiothoracic Minia University Hospital in Egypt. The study published in 2024 in the Malaysian Journal of Medical Research (MJMR) included all Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD) patients presenting to the emergency department (ED) with respiratory acidosis, PaCO2 greater than 45 mmHg and a pH lower than 7.35. The study also included patients presenting to the ED on NiPPV from another hospital. The study excluded patients with asthma, end stage cancer, respiratory or cardiac arrest and hemodynamic instability among other criteria.
Seventy-four patients meeting the inclusion criteria were enrolled and randomized to either high velocity nasal insufflation (HVNI) with a starting flow rate of 35L/min, an FiO2 of 1.0 and temperature from 35°C-37°C or Non-invasive Positive Pressure Ventilation (NiPPV) with initial parameters of 10:20 cmH2O for inspiratory positive airway pressure, 5:10 cmH2O for the expiratory positive airway pressure, and 1.0 for the FiO2. The researchers sought to compare the two groups based on the ventilatory effect and therapeutic impact of each modality.
The objective for both modalities was to increase patient comfort as evaluated by the clinician, relieve respiratory distress by reducing respiratory rate (RR) < 25 breaths/minute and to keep saturation levels over 88%. Arterial Blood Gas (ABG) samples at 0, 1h, 2hrs, 6hrs, 24hrs and on discharge were collected and analyzed. Treatment failure was defined as the need for invasive mechanical ventilation or shift to the other device.
34 of the 74 included patients were randomized to HVNI and 40 patients to NiPPV. There were no statistically significant differences between the two groups regarding RR, pH, PaCO2 and PaO2 on admission, after 1hr, 2hrs, 6hrs, 24hrs and on discharge. For intra-group comparison, there was statistically significant decline in RR and PaCO2 after 1hr compared to RR and PaCO2 on admission, and after 2hrs, 6hrs, 24hrs and on discharge compared to baseline either in the NiPPV group or in the HVNI group (p<0.001). (Figures 1 & 2).
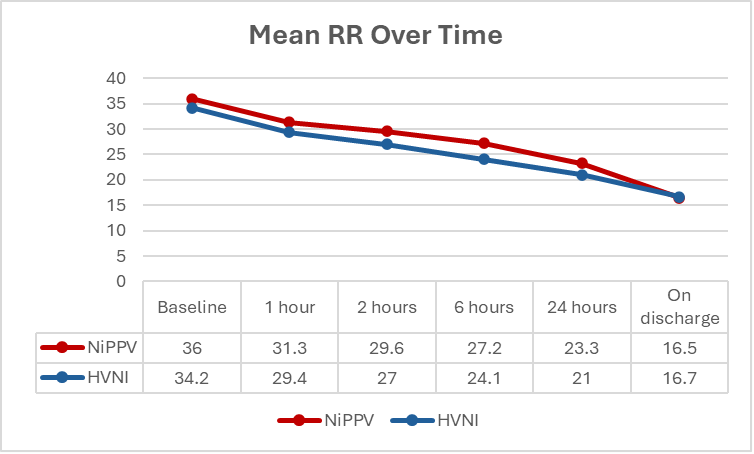
Figure 1: Mean respiratory rate (RR) over time for both groups.

Figure 2: Mean PaCO2 over time for both groups.
The results also showed a statistically significant increase in the pH and PaO2 values after 1hr compared to pH and PaO2 on admission, as well as after 2hrs, 6hrs, 24hrs and on discharge compared to baseline either in the NiPPV group or the HVNI group (p<0.001). (Figures 3 & 4).

Figure 3: Mean pH over time for both groups.

Figure 4: Mean PaO2 over time for both groups.
The total duration of hospital admission was greater in the NiPPV group (mean = 17.5 days) than in the HVNI group (mean =15 days); (p=0.03). Regarding shift to another device, 3 cases shifted from NiPPV to HVNI (7.5%) compared to 11 cases shifting from HVNI to NiPPV (32.4%); (p=<0.001). There were no significant differences among the 2 groups in success rate, duration of device application, need for intubation (intubation rate was 17.6% in the HVNI group and 25% in the NiPPV group), duration of invasive mechanical ventilation, duration of ICU stay, intubation after device shift, in-hospital mortality and 30 days mortality (p value >0.05).
The authors conclude that HVNI is effective as a ventilatory support in AECOPD patients presenting with acute type II respiratory failure with non-inferior success compared to NiPPV. The authors also caution that more research is required to confirm these results.

All Clinical Research
Go back to the Clinical Research table of contents
Mask-Free Respiratory Support
Vapotherm High Velocity Therapy
CAUTION: US Federal law restricts this device to sale by or on the order of a physician. Indications, contraindications, warnings, and instructions for use can be found in the product labelling supplied with each device or at https://vapotherm.com/resources/support/precision-flow-reference/. For spontaneously breathing patients. High Velocity Therapy (HVT) does not provide total ventilatory requirements of the patient. It is not a ventilator. Decisions surrounding patient care depend on the physician’s professional judgment in consideration of all available information for the individual case, including escalation of care depending on patient condition.